Though this is not a perfect rule, when you hear “-oma” on the end of a word, it usually suggests cancer of some sort.
Used alone with a prefix that designates a tissue type, “-oma” classically has a connotation that suggests a benign tumor rather than a malignant one. (Ex: adenoma = benign tumor of a glandular epithelial cell type; chondroma = benign tumor composed of cartilage.) That’s not always true, though. So don’t depend on it.
Let’s try it!
“-oma”-words that have to do with tumors:
Carcinoma – This is a general term for a neoplasia (neo = new; plasm = growth) that originates from an epithelial cell type. (The body is made of four main cell types: epithelial, connective, muscle, and nerve.)
Epithelial cells cover things, secrete things, and transport things from one side of a membrane to another. Epithelial cells constitute the skin, the linings of the mucous membranes, glands, the lining of the bladder, and the linings of various ducts and tubes within the body.
After age 45, more than 90% of all tumors are derived from cells of epithelial origin.
The Culprits.
Lymphoma – Classically used to describe neoplasias of white blood cells (immune cells) that tend to stay in discrete masses. (There’s some overlap with “leukemias”, which are neoplasias of white blood cells that classically involve the bone marrow and often present with tumor cells in the blood.)
This is what a “mantle cell lymphoma” looks like under a microscope. I saw a patient with this type of lymphoma just last week.
Lipoma – A benign tumor composed of fat cells. (Lipos = fat)
There are also malignant tumors composed of fat cells, known as liposarcomas. My first-ever surgery as a third-year medical student was actually a liposarcoma removal. The thing was beach-ball-sized. And guess who got to hold it out of the way as the surgeons removed its connections to the patient’s abdomen? That’s right! My first surgery experience consisted in standing with my arms completely wrapped around a heavy, gigantoid tumor made of fat cells. For at least four hours.
It looked a little like this:
Have you hugged your liposarcoma today?
Incidentaloma – This is a tumor (or other finding) found by coincidence on an imaging study that was actually looking for something else entirely. These can be benign or life-threatening, and are often completely asymptomatic (a = without; symptomatic =….well, you got it).
This was an MRI study of the lumbar spine (the stack of rectangular objects in the middle). This patient also has 'arrow sign': the radiologists are drawing attention to a mass around the distribution of the left adrenal gland. Surprise!
“-oma”-words that don’t necessarily have to do with tumor (except maybe in the Latin sense of the word):
Glaucoma – This is a group of eye diseases characterized by certain changes in the visual field and the cup of the optic nerve. Often associated with high pressure inside the eye.
This is what a doc is looking at when they shine a bright light into your eye. This is what the back inside surface of the eye is supposed to look like.
This is glaucoma. Notice that the optic nerve (the circle in the middle) looks like a cup; the indentation in the middle is far bigger than it’s supposed to be.
Stoma – This is an opening in the body that may resemble a mouth. Sometimes refers to a hole made in the body and maintained to allow drainage.
Stoma
MOMA – This is a museum in New York.
It’s pretty swell, but I don’t think that counts.
Now go forth and understand some doctor-talk!
References:
Robbins and Cotran. Pathologic Basis of Disease. 7th edition. Elsevier, 2005.
Junqueira, Luis Carlos; Carneiro, Jose. Basic Histology: text and atlas. 11th edition. McGraw-Hill, 2005.
The contents of this site, such as text, graphics, images, and other material contained on the Site (“Content”) are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this Site!
If you think you may have a medical emergency, call your doctor or 911 immediately. This blog does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the Site. Reliance on any information provided by this blog, or other visitors to the Site is solely at your own risk.
The Site may contain health- or medical-related materials that are sexually explicit. If you find these materials offensive, you may not want to use our Site. The Site and the Content are provided on an “as is” basis.
If you use this as if it were real medical information, I will come to your home and hug your beach-ball for at least four hours. It will almost certainly confuse your children.
You need your character to unexpectedly drop dead, with no warning. You need a good, plausible medical reason for this to happen.
You’ve come to the right place, evil killer of beloved characters! ::ahemGeorgeRRMartincough::
Note: It might help to review “I ❤ the Lub-Dubber”, the post about the cardiovascular system.
Another note: While you’re reading this, remember that the first priority of a first responder to a medical emergency is their ABCs: Airway, Breathing, and Circulation. This is because the body cannot survive without proper oxygenation. Now, without further ado:
Here are six medical conditions that could cause your character to suddenly drop dead.
Aortic Dissection:
What it is: The aorta is the main artery that leads out of the heart. Like all arteries, its walls are made up of multiple layers. Sometimes, a tear occurs in the inner layer. This allows the high-pressure blood in the aorta to push itself in between the layers, “dissecting” the inner layer away from the other layers.
Why the character will die: There are a couple of problems that this can cause. A main one: the flap of the inner layer can cover up the openings to arteries that lead out of the aorta. This can lead to ischemia (oxygen deprivation) of whatever was at the other end of the artery, including the brain or even the heart itself.
Make it plausible: Your character probably has high blood pressure. They might describe a sudden onset of incredibly severe, “tearing” chest pain, which classically radiates to the back.
Hypertrophic Cardiomyopathy:
What it is: A genetic disorder of the heart muscle causes the walls of the left ventricle to get really big and thick. (hyper = over/above, troph = grow, card = heart, myo = muscle, path = feeling/suffering).
Why the character will die: There are a number of ways this can cause problems. (1) In one set of problems, the passage to the aorta (also known as the left ventricular outflow tract) gets blocked by the oversized walls of the left ventricle. No blood gets out of the heart, and therefore nothing in the body can get oxygen. This may happen when they’re at rest, but more often happens when they’re exercising. (2) The electrical system of the heart may be out of whack; that would make it prone to arrhythmias. (See the section on Cardiac Arrhythmia) (3) The heart muscle itself could be less-than-functional: either it doesn’t pump well, or it’s bad at relaxing so it can’t fill up after it pumps.
Make it plausible: Your character is a young, fit athlete. He or she suddenly drops dead while exercising. A member of their family (a parent, for example) may have died suddenly due to the same reason.
Massive Pulmonary Embolism:
What it is: Something blocks off the circulation of blood into the lungs. (Pulmonary = lungs; Embolism = the blockage of a blood vessel with some kind of material.) It’s often a blood clot, but it can also be fat, air, or even tumor material.
Why the character will die: The blood will get backed up from the blockage. This causes a severe drop in blood delivery (measured by blood pressure) to the body, with an increase of pressure behind the blockage. This can cause failure of the right heart (which can’t pump against that kind of pressure). No blood oxygenation, and compromised circulation. Bad news.
Make it plausible: Emboli that come from blood clots are often from deep vein thromboses, or clots that form in the deep veins (often of the legs). There are some risk factors which make it more likely that your character may develop a pulmonary embolus. These include recent immobilization, recent surgery, stroke, paralysis, chronic heart disease, and cancer. Your character may be obese, may have high blood pressure, and may be a smoker.
Cardiac Arrhythmia:
What it is: A disturbance in the electrical pathways in the heart. This can cause the interruption of proper coordinated pumping in the heart muscle; some arrhythmias can lead to sudden death.
Why the character will die: The pumping of the heart muscle becomes uncoordinated. This results in inadequate filling and/or emptying of the chambers of the heart. Which means that the heart can’t properly pump blood out to the rest of the body. Which means the rest of the body doesn’t get any oxygen.
Make it plausible: There are a LOT of reasons why people get arrhythmias. Everything from being born with extra pathways that run the electrical activity of the heart in a circle, to the sequelae (after-effects) of a heart attack, to drug toxicity, to irregularities of ion flow in the cells of the heart. Research is your friend in this case.
Berry Aneurysm, Sub-Arachnoid Hemorrhage:
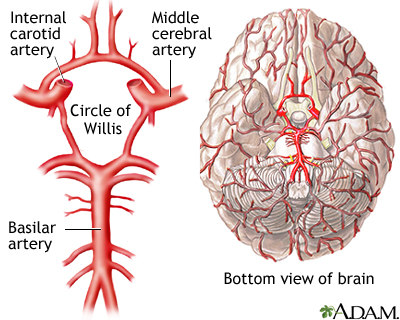
What it is: One of the blood vessels in the brain, most likely in the Circle of Willis…
…develops an out-pouching called an aneurysm.
Your character may have been born with it, or they may have acquired it at some point during their life. The acquired ones seem to be more likely to cause problems.
Why the character will die: The aneurysm itself probably doesn’t make much trouble…but it runs the risk of bursting, causing a major brain bleed. The resulting bleed is called a sub-arachnoid hemorrhage, after the space that your character bleeds into. Note: I hyphenated “sub-arachnoid” to make it easier to read and understand. (sub = under, and “arachnoid” refers to the arachnoid mater that surrounds the brain tissue.) It’s usually written as “subarachnoid”. Sub-arachnoid hemorrhages are dangerous; around 50% are fatal.
See that white starfish shape in the middle of the brain? That ain't supposed to be there. That's blood in the arachnoid space. Seeing that on a head film would sure squeeze the heck out of your adrenals (as my cardiology preceptor would say).
Make it plausible: Your character will likely have high blood pressure, and will probably smoke cigarettes. Your character may also be a heavy drinker. A family member (parent, sibling, grandparent) may also have died suddenly from the same cause, but not always.
Are there any that AREN’T cardiovascular?
Cardiovascular causes do seem to be pretty prominent, don’t they? Strokes, aneurysms, emboli, heart attacks…they all have to do with the heart and blood vessels.
The only non-cardiovascular cause of potentially instant-ish death I can think of off the top of my head is anaphylaxis. Which, um, has a cardiovascular cause of death. ::sigh:: I’ll include it anyway.
Anaphylaxis
What it is: Anaphylaxis is an overwhelming allergic reaction to a triggering factor. The substance can be anything from a bee-sting to a food item to a medication. (I couldn’t find any pictures that satisfied me for this condition; there’s just too much going on to accurately represent it with one image.)
Why the character will die: There are two main problems that may result in death from anaphylaxis. (1) There is a certain balance of where the fluid in your body likes to stay, be it in blood vessels or in the general body tissues. In anaphylaxis, there is a massive shift of fluid out of the blood vessels and into the body tissues. That results in the compromise of the cardiovascular system (can’t escape it, can we?), which endangers the perfusion of oxygen to the brain and tissues. (2) There is a significant amount of tissue swelling involved, and this can extend to the breathing passages. This results in a blockage of the airway. That means that the character will not be able to get enough air into their lungs to properly oxygenate their blood. And you have the same problem.
Make it plausible: A food allergy will often result in airway compromise and respiratory arrest. A venom allergy (beesting, etc.) will often result in cardiovascular compromise. Also, there are some age correlations with triggering factors, though pretty much anyone can react to pretty much anything regardless of age. That said,
–Adolescents and young adults are at most risk of death from food reactions.
–Middle-aged adults are at most risk of death from venom reactions
–Older adults are at most risk of death from drug reactions
Last note today, I promise: Any one of these can be fatal or not, depending on the person and the situation. Sell it how you want to sell it, but make sure you set up the situation properly for plausibility purposes.
The contents of this site, such as text, graphics, images, and other material contained on the Site (“Content”) are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this Site!
If you think you may have a medical emergency, call your doctor or 911 immediately. This blog does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the Site. Reliance on any information provided by this blog, or other visitors to the Site is solely at your own risk.
The Site may contain health- or medical-related materials that are sexually explicit. If you find these materials offensive, you may not want to use our Site. The Site and the Content are provided on an “as is” basis.
If you use this as if it were real medical information, these posts will be published by dead drop. You probably don’t have access to the drop point.
“(The heart), nurtured in the seas of rebounding blood,
where most especially is what is called thought by humans,
for the blood round the heart in humans is thought.” –Empedocles
If you held a gun to my head and asked me what my favorite organ was, I’d probably crap my pants and beg you not to shoot me.
But if you were really serious about getting an answer to your question, I’d probably tell you that I absolutely love the heart. You know, after you took the gun away and I got cleaned up a little bit.
Not just because it pulled a fast one on some of my favorite philosophers. Though I gotta admit, I do love watching the history of knowledge unfold through trial-and-error. But seriously, I think it’s functionally and aesthetically the prettiest organ in the body.
(Kidneys are cool, too, but I get a complex about brainless objects that are nonetheless smarter than I am.)
Wanna see something beautiful?
This shows an MRI of a heart beating. Just watch it for a minute. It’s gorgeous. PS: Can you identify the piano piece? Thanks, Interwebz!
Your heart is basically a chunk of muscle that contracts in a really cool way to push your blood around your body. The heart is the center of the circulatory system. That’s the system that’s responsible for getting important groceries from one place to the other in your body: glucose (cell food), oxygen, etc. It also takes out the trash: urea, carbon dioxide, and all those other yuckies that would otherwise gum up the works. And poison you and stuff. Basically, anything that needs to get from one place to another goes through the circulatory system.
It’s like the internet and the transportation system combined: it’s a series of tubes! And through the tubes goes everything from gasses to sugars to hormonal messages.
What’s the setup for the body’s circulation?
The circulatory system is organized like an infinity sign or a figure-eight, with the heart at the cross-over point. One loop is the pulmonary loop that goes to the lungs, and the other is the systemic loop that goes to the rest of the body and all of the organs.
Okay, now we’re red blood cells! We’re going to take a trip through the circulatory system!
Can we go to Hawaii instead?
No.
Why not?
Because we’re red blood cells. And we’re going to take a trip through the circulatory system.
There are red blood cells in Hawaii. And, if I recall correctly, there are also circulatory systems in Hawaii.
. . .
. . . You’re right.
Yes. Yes, I am.
Okay, then. We’re red blood cells. In Hawaii.
Hooray!
Let’s arbitrarily start our journey right before we get into the heart.
Our job as red blood cells is to carry oxygen (O2). We’ve just popped the O2 off of our hemoglobin at our last stop, and loaded up with carbon dioxide (CO2). We want to get the CO2 out of the body, and pick up some more oxygen so we can make another delivery.
We enter the heart through a big vein called the vena cava. The vena cava empties into the first chamber of the heart, the right atrium.
The right atrium is a little room made of contracting muscle. Its job is to top off the right ventricle, which is the main pumping chamber of the right side of the heart. The atrium and ventricle are separated by a one-way “door” called the tricuspid valve (so called because it has three “cusps”, or leaflets.)
So, the right atrium is going to give a squeeze, and propel us through the tricuspid valve into the right ventricle. The right ventricle is relaxing after its previous squeeze; that’s called “diastole”.
It’s very. . . um. . . muscular in here.
Yeah, these pumping chambers are made completely of bundles of muscle fibers. That’s important, because the heart needs to put some force behind its squeezes.
The right ventricle’s job is to provide the force that pushes us through to the lungs, so we can exchange our load of CO2 for O2. To get there, we have to go through another one-way “door” called the pulmonic valve, and through a series of splitting tubes called the pulmonary arteries.
Note: Some people are taught that “arteries carry oxygenated blood and veins carry de-oxygenated blood.” This isn’t entirely correct. By definition, arteries carry blood away from the heart and veins carry blood toward the heart. In the pulmonary (lung) circulation, arteries carry de-oxygenated blood, and veins carry oxygenated blood.
So the right ventricle gives a good squeeze! This is called “systole”. And now, we shoot through the pulmonic valve. We travel through the pulmonary arteries, and end up in the tree-branch-like system of the capillaries of the lungs.
These capillaries are tiny blood vessels that are only wide enough to let one blood cell through at a time. So let’s hold hands so we don’t lose each other, and squeeze on through. We’re close enough to the alveoli (the tiny bags that fill with air when you breathe) that we can drop off our CO2, and load up some O2 for our next delivery run.
Alveoli
And now we’re set to move on!
After we traverse the capillaries, we find ourselves in a reverse-tree-branch-like system: the tiny capillaries are coalescing to form larger and fewer vessels, called the pulmonary veins. We’re on our way back to the heart!
When we reach the “trunk of the tree”, we’re in the pulmonary vein. This empties into the left atrium. The function of the left atrium is a lot like the function of the right atrium. Its job is to top off the left ventricle.
The one-way “door” between the left atrium and the left ventricle is called the mitral valve. So, the left atrium is going to give a good squeeze, and push us through the mitral valve into the left ventricle. The left ventricle is relaxing; it’s in diastole.
And we’re stunned. We’re just flabbergasted.
Um…why?
Remember the right ventricle? The main pumping chamber that pushed us into the lungs?
Yeah?
It was pretty strong, right?
Yeah, it gave us a good push. It took some force to do that.
Well, strength-wise, the left ventricle could EAT THE RIGHT VENTRICLE FOR BREAKFAST. You know, not even breakfast. Maybe even just a midmorning snack. The left ventricle is HUGE!
Look how much bigger the Left Ventricle is on cross-section!
Maybe it’s compensating for something.
Yeah, it is! It’s compensating for the fact that it has to provide enough force to squeeze blood THROUGH THE ENTIRE BODY!
eep.
So we’ve just come through the mitral valve, and we’re chilling in the left ventricle. In front of us, we can see the aortic valve, which is the one-way “door” that leads out of the heart into the main artery of the body, the aorta.
And I can feel the left ventricle getting ready to squeeze. Get ready for systole!
Um . . .
It’s building up! It’s gonna be a big one!
Ummm. . .
What? What’s wrong?
Stop the circulatory system! I wanna get off!
Too late! Hold on, we’re into SYSTOLEEEEEEEEEEEEE!!!!!!!!!!!!!!!!!!!
AAAAAAAAAAAAAAAAAAA!!!!!!!!!!!!!!!
Observe my sloppy Photoshopping on the way!
We’re sailing through the aortic valve and into the aorta! We have a lot of places we can go to deliver our oxygen now, and our first choice comes up almost immediately: the coronary arteries, which supply oxygen to the heart muscle. These guys are really important; if they get blocked off, you get a myocardial infarction (myo = muscle, card = heart, infarct = oxygen deprivation), also known as a heart attack.
But there’s plenty of blood heading into the coronary arteries; let’s stick with the aorta for a bit.
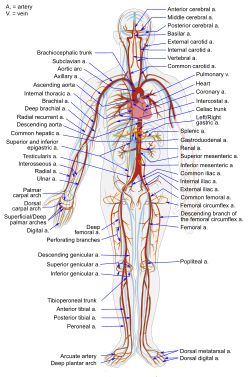
The Aorta has many branches; each one is an artery going to a different part of the body. The carotid arteries head up to the brain. The renal arteries come off of the aorta as it descends into the abdomen, and supply the kidneys. Just look at all these options!
So, pick a part of the body, and we’ll go there and dump our O2. Then we’ll pick up any CO2 it needs to get rid of.
Let’s go to the fourth toe on the right foot.
Um…sure. Good a place as any, I guess. Any particular reason?
How often does that guy get any attention?
Okay, fair enough. So we’re going to travel through the arterial tree, traveling through smaller and smaller arteries until we reach the bed of capillaries that supplies the (ahem) fourth toe on the right foot. Each cell is within striking distance of a capillary, so it can have access to supplies and waste removal services.
Now pick a cell and unload your O2 so it can keep doing its job. And go ahead and pick up some CO2, too.
Got it. Let’s blow this popsicle stand.
Awesome!
So, now we’re going to head out the other side of the capillary bed. The blood vessels are coalescing again, making bigger and bigger vessels. This is the venous part of the systemic circuit.
venous?
Venous.
Venous!
Hee hee! VENOUS!
VENOUS!
Okay, okay, you win. I can’t shout any louder without getting people confused as to who’s talking.
Ooh, self-referential font humor. I’ll declare victory anyway.
Good job.
Okay, we’re headed through the veins on the way back to the heart. The veins coalesce into the vena cava. . . and we’re back where we started.
From here, we’d pass through the right heart into the pulmonary circuit, and then pass through the left heart into the systemic circuit, and around and around and around.
But that would make me a little dizzy, and plus, this post is a monster as it is.
So, that’s the mechanical setup of the circulatory system. It’s just a series of pumps and pipes. If you want to mess with it. . . just think about what happens when a system of pipes gets backed up. Or if the valves start allowing back-flow, or if they get too stiff to allow much flow. Or if the pump becomes weak and inefficient. Or if the pressure gets too high for the pump to push against.
But before I sign off for today, wanna see something gorgeous?
This is the procedure I spent the vast majority of last month observing. It’s called a cardiac catheterization. We’re taking pictures of the coronary arteries by shooting a little bit of opaque dye into them under an X-ray machine. This test looks for blocked or narrowed coronary arteries, which could cause a heart attack if they’re not opened up.
Man, I could look at those forever.
What’s your favorite organ system?
Source:
Cohen, Curd, and Reeve. Readings in Ancient Greek Philosophy. Second edition. Hackett Publishing Company, 2000.
Pictures:
The contents of this site, such as text, graphics, images, and other material contained on the Site (“Content”) are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this Site!
If you think you may have a medical emergency, call your doctor or 911 immediately. This blog does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the Site. Reliance on any information provided by this blog, or other visitors to the Site is solely at your own risk.
The Site may contain health- or medical-related materials that are sexually explicit. If you find these materials offensive, you may not want to use our Site. The Site and the Content are provided on an “as is” basis.
If you use this as if it were real medical information, I’ll take my circulatory system to Hawaii without you.
I love this song. I love the almost unforgivably peppy bounciness of the thing, and I adore how the brashness of the ascending modulations near the end of the song just pulls my mood right up with them.
But I also enjoy (some of) the lyrics: “Stand in the place where you work…” and think about it for a minute. And “wonder why you haven’t before.”
I do that all the time, actually. As a writer, I’m a constant people-interacting-with-surroundings-watcher. And by all that is good and writerly, there is no more fascinating place to observe humanity than in a hospital.
I’m not even talking about the patients, or their families, though you will never see a more honest cross-section of humanity anywhere else.
I’m talking about the staff.
If you’ve worked in any kind of service profession, you know how much it sucks when one of your customers is having a bad day. They take it out on you, right? And it can completely ruin your day.
In my job, EVERY PERSON I INTERACT WITH is having one of the worst days of their entire life. They’ve just been told they have cancer. Their child may not live to see the sun rise in the morning. They haven’t slept in a real bed for days, months, or years, and they’ve been poisoning themselves with nothing but hospital food. They’ve been cut open and had a leg or a kidney or a section of their intestines removed from their body. They’re in pain, they’re scared, they’re lonely, they’re dying.
That’s baseline.
Now think about the people who are there every day. Who not only interact with patients and families in a pleasant and patient manner, but also are expected to work miracles, teach complex concepts, learn complex concepts, be scientifically brilliant as they make life-and-death decisions, and get along well with their co-workers. On 30-hour shifts. With a sometimes abusive patient load. In danger of catching hepatitis or HIV from a slip of the wrong needle.
Stand in the place where you work, indeed. In an environment like that, your very survival might depend on your team.
You’re exaggerating.
Well, yeah, maybe about the “very survival” part. (I always thought the “your very survival” was a silly grammatical construction, by the way. You can’t say it except in an overdramatic exaggeration.) But I’ve been on good medical teams and bad medical teams, and you wouldn’t believe the difference it can make.
If you’ve ever been in a hospital (at least, a teaching hospital), you’ve probably been the focus of an experience in which ENTIRELY TOO MANY PEOPLE IN WHITE COATS crowd around your bed near the beginning of the day (probably waking you up in the process), talk about stuff incomprehensibly, and leave. You might see those people individually over the course of the rest of the day, each breezing in and out with some random task or question. You probably have no idea what anyone’s name is.
That’s your medical team.
So here’s the basic structure of a medical team, at least at the teaching hospitals I’ve been working in. Try picking it apart next time the flock of white coats surrounds you while they round on you. Remember that there can be pretty much any combination of these roles on a typical team.
At the head you have the Attending Physician. The head honcho! The big cheese! That “here” whence the fabled “buck” doeth “stop”! (Is that a proper use of “whence”? I couldn’t decide, so I figured I’d just run with it.) The Attending is in charge of the service, and is ultimately responsible for the patient’s treatment. If there’s one relatively much older person in the group, that’s most likely the attending.
Sometimes a service will include a Fellow. (This can be a guy or a girl; it’s the name of a position in this case. Not replaceable with “feller”. Believe me.) The Fellow is a doctor who has completed medical school and residency, and is specializing further in their field: cardiovascular medicine, pulmonary critical care, endocrinology, or whatever else. I don’t know exactly how fellowships work; I’m not there yet. But I love having Fellows on the service; they are the most knowledgeable on the medical team (with the exception of the Attending), and they tend to be a little more accessible for questions. All of the Fellows I have been on service with have run very, very good teams.
Next on the ladder, we have the Resident(s). Residents are doctors who have completed medical school and are in their “apprenticeship” period. This is the time when they really learn how to practice medicine: decision-making, knowledge base, and leadership. The Resident on the team is usually responsible for the ultimate design of the treatment course (with the approval of the Attending and perhaps the assistance of the Fellow). The Resident is also in charge of managing the team that is taking care of his patient, and is responsible for making sure the day-to-day tasks of patient care are taken care of. The quality of a patient’s treatment really depends on the quality of the Resident. I’ve worked with fantastic Residents and awful Residents. They can really make or break a team.
And one step down are the Interns. This is actually the step I’m about to take. Internship is the first year of residency; Interns are full doctors for the first time. They are often the workhorses of the medical team. They are the patient managers. They are the hands that accomplish the tasks of patient care. They are often the ones who take calls from nurses, especially overnight. From everything I’ve heard, intern year is brutal. And the learning curve is steep. This is both exciting and terrifying to me.
In my experience, Interns tend to be the most cynical and angry people on a medical team. They work HARD, and it’s hard work. Under massive amounts of stress. For very little pay. Here’s a song that pretty much catches the general attitude of intern year, at least as I’ve seen people react to it. Note: I’m actually rather hesitant to post it, because it’s very patient-unfriendly…but it’s honest, even if it’s angry. And it’s very, very angry. Not safe for work.
Next (sometimes), you have Sub-Interns. These are fourth-year medical students. Like me. We try to act like Interns. But we have less ultimate responsibility, so ultimately less existential stress.
And then, the Medical Students. These can be either third- or fourth-year students, depending on the setup of the team.
I think this video pretty much says it all:
If you’re lucky, your team might have a Pharmacist and/or a Nurse Practitioner and/or a Physician’s Assistant on it. These people are freaking life-savers. For everyone, patients and staff alike.
People rotate in and out of the teams on a biweekly or monthly basis, depending on the service and on the schedules of the team members. So a medical team is in a state of constant flux. This can be a good thing or a bad thing; it breaks up bad teams after a while so you don’t have to work with malignant people forever, but it breaks up the good teams, too.
So where does the “high-stakes hippie love-fest” come in?
I love working on a medical team. For whatever reason, it just suits me. And I love it when the team really gels, even when it’s destined to break up at the end of the month.
I’ve been on teams where people practically ran down the hall, jostling good-naturedly for the privilege of holding the door for the rest of the team during rounds.
I’ve been on teams where, first thing after rounds, everyone descends on the post-call team member and asks to help with her work so she can go home sooner after she’s worked 30 hours… no matter how much work they have to do themselves.
I’ve also been on a team where the resident actively undermined his team members, not even always to make himself look good.
I really do prefer the functional teams. I guess I’m a little sensitive to group dynamics, and it just makes life easier when everyone supports each other, respects each other, and generally gets along.
Because the hospital environment can be physically and emotionally as dangerous as a world on the other side of a Stargate. And facing that kind of peril, it’s so much nicer to step through with people who have your back.
What is your work environment like (if you have a day job)?
Note: This post does not include anything about medicine. Is that okay?
For whatever reason, I am completely caught up with all the shows I have chosen to follow. Which tells me I haven’t been writing enough recently.
(You know, I was completely TV-show-less for about five years. What happened? I blame med school; sometimes you just can’t write when you come home from the hospital. And you just can’t sleep either. I also blame the internet, for making TV shows accessible to me even though I don’t own a set. I also blame the fact that there’s some really neat writing going on in TV-land recently. Sometimes it’s hard to turn away.)
Anyway, I don’t like being caught up. When I come home, I want to turn my brain off and be told a story that re-energizes me in the way that the best stories can. But I have to wait until people start putting out new episodes again.
But this spate of TV-show famine got me thinking about what it is about a TV show that sucks me in. Because I’ve become hooked on a number of shows practically against my will, and I’ve also bounced off a number of shows that other people seem to really like.
Here are some shows that I’ve deeply enjoyed. (In no particular order.)
Firefly
The West Wing
Pushing Daisies
Warehouse 13
Leverage
Doctor Who
Stargate SG-1
Studio 60 on the Sunset Strip
The Big Bang Theory
Sliders
Scrubs
Here are a few shows that I’ve recently tried, but have been unable to get enthusiastic about.
Dollhouse
Battlestar Galactica
Stargate Universe
I realized that the first group of shows have something in common: They’re centered around a small group of people who genuinely like and respect each other (with some petty-but-affectionate sniping allowed, to flavor the interactions.)
The second group of shows have groups of characters who seem to be in constant, negative-vibes, uncomfortable conflict.
Now, conflict definitely drives a storyline. It’s important. But you’d be hard-pressed to deny that there’s a good amount of conflict in any of the shows in the first group. So what’s the difference?
I’m not much of a sports fan, and I certainly don’t have any loyalty to any sports team (much to the chagrin of my friends who want to bait me across state lines when there’s a classic rivalry). But I do enjoy the occasional game between evenly-matched teams. And I am always secretly rooting for the basketball teams that have the most complex passing patterns; the teams that look like they’re moving as a single organism.
It looks like I have a preference for conflict external to the central group rather than internal. I love watching people play as a team. And that seems to bleed over into my story preferences.
I’m definitely not saying that there can’t be any internal conflict; I was blown away by the genuine-ness of the fights that the crew of Serenity had with each other. But their fights were always driven by a deep streak of “I’m fighting because I give a damn about what happens to all of us.”
Contrast this with the shows in the second group, which also had a group of characters with problems to solve. . . but they work against each other as much as or more than they work against their various antagonizing forces. With very sparse exception, there’s no mutual affection anywhere to latch onto. I just don’t LIKE anyone enough to root for them.
I guess there’s only so much angst I can take. Give me a show with a bunch of people who have each other’s back. Give me a group to root for as they take on the world. Not because it’s their job. I mean, it can start there. But it really has to develop into true I-give-a-damn-itude in order to hold my fascination.
My favorite shows, therefore, seem to be the high-stakes hippie love-fests.
Note: Oh, man. It looks like I was talking about medicine after all. I’ll tell you why later on.
But how about you? What do your favorite shows/stories seem to have in common? And how does your work use (or fail to use) that commonality?













.jpg)





























.svg/350px-Diagram_of_the_human_heart_(cropped).svg.png)






{kind=link}
{kind=link}