In honor of the fact that I’m rotating through Neurology at the moment, I’m proud to present…
NERVES!
(In case you don’t read Morse Code and were too lazy to google it, that’s what the title says.)
So, nerves are super-cool.
Here’s a picture of one, so you can join me in basking in the coolness of nerves.
Are you basking?
What’d I tell you? Coolness personified.
Well, maybe not personified….but if you squint closely, you may find yourself glancing at your neighbor and having a shift in perception, suddenly seeing his shape described only by a network of white, filamentous strands, as if he were a sculpture of spiderwebs….
Only me?
Darn.
Well, that’s okay. I also subconsciously judge people based on how easily I could start an IV in the veins on their hands.
(The study of medicine engenders its own special flavors of crazy.)
Anyhoo. NERVES!
A nerve cell is called a neuron. That’s the cell in whose coolness we were basking, up there a minute ago.
The job of a neuron is to pass information along, in the form of an electrical signal. (The way this happens is super-cool, and warrants its own post, so stay tuned. For right now, we’ll just talk about how they’re arranged.)
There are three parts to any neuron.
The dendrites (from “dendron”, which means “tree”) are the tree-branch-like projections off of the central cell body, also known as the soma or perikaryon. The dendrites collect impulses from surrounding neurons and send them to the perikaryon. There are usually a lot of dendrites on a neuron, making it easier to collect a LOT of information.
(Dendrites are probably the coolest things in the human body, because they like to rearrange themselves like crazy, making a dynamic structure that allows us to learn and remember things, and adapt to changes and all kinds of other important things like that.)
So, a neuron receives signals through its dendrites. But what if it wants to say something to the other nerves in the area? That’s where the third part of a neuron comes in, the axon.
Axons are incredibly cool structures, too! There’s a conical process on one end of a perikaryon called the axon hillock, and that’s the staging platform that shoots off the axon, a long, cylindrical filament that keeps its diameter for practically its entire length (whereas the dendrites tend to taper off). Axons are responsible for carrying information away from the perikaryon, toward whatever it’s supposed to connect with and talk to. Wherever it is.
(Think about how far away the tip of your toe is away from the end of your spinal cord [it’s a little above the level of your iliac crests, if you remember from this post. ] A nerve axon has to run that entire distance to carry its signals! They’re LONG, man!)
Okay, a little more terminology, then I’m calling this post a wrap and going to bed. And then we’ll get to the REALLY incredibly cool stuff in the next couple of posts.
The connection where nerves can talk to each other (or to muscles or gland cells or whatever) is called a synapse. Axons can form synapses with cell bodies, dendrites, or even other axons. For clarity purposes when describing nerve connections, a neuron sending a signal toward the synapse is called “presynaptic”, and a neuron that receives the signal from the synapse is called “postsynaptic”.
Makes sense, right?
Synapses are oases of awesome in a desert where the sand is made of unabashed coolness. They might get their own post. Or a couple. We’ll see.
Anyhoo. NERVES!
Axons are covered with a nifty stretch of jointed insulation, called a myelin sheath. More about that, too. Later.
I know you can’t wait. I hardly can either.
But I’m pushing bedtime as it is.
Man, I’m a geezer already.
But that’s okay. At least you can read this at three in the morning, if you want.
Because your nerves make it possible.
NERVES!!!
Pictures:
Resources:
Junqueira, Luis Carlos; Carneiro, Jose. Basic Histology: text and atlas. 11th edition. McGraw-Hill, 2005.
The contents of this site, such as text, graphics, images, and other material contained on the Site (“Content”) are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this Site!
If you think you may have a medical emergency, call your doctor or 911 immediately. This blog does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the Site. Reliance on any information provided by this blog, or other visitors to the Site is solely at your own risk.
The Site may contain health- or medical-related materials that are sexually explicit. If you find these materials offensive, you may not want to use our Site. The Site and the Content are provided on an “as is” basis.
If you use this as if it were real medical information, I’ll bask in the cool awesomeness all by myself. Didja hear me? ALL BY MYSELF! (So there.)
I’m a little uneasy about the whole idea of writing a post about using cancer as a fictional tool, because it’s such a devastating disease to patients and family members. But it is an important disease type, and I see it used everywhere in stories. Basically, whenever someone wants to deliver an emotional wallop. So…I’m going to give you some info on it.
But remember, cancer sucks. There’s nothing about cancer that doesn’t suck. And chances are, everyone in your audience will either know someone with cancer or have it themselves. So when you write about cancer, as with all diseases, try to remember that these are the things that destroy lives and tear families apart. Please write with a conscience.
And please take a moment to send some good vibes to anyone who is suffering from cancer, and to their families and friends. They could really use it.
And now, to the fictional world. As I’m sure you’ve seen in any number of stories, this collection of diseases can make a very useful tool for plot and/or character development.
Cancer is a general term to describe a type of disease: the runaway growth of a cell line. (This is also called a “neoplasm”, which means “new growth”.) Cancer can happen in practically any cell of the body. It’s a huge collection of diseases.
On the fiction end of things, cancer is a remarkably versatile disease type. So you can use it for many different situations, with practically any character.
What is it?
Cells have a mechanism for replicating themselves, dividing into daughter cells.
As you might imagine, there are a lot of brakes in place, so that cells divide only on the proper schedule. Because if the brakes are broken, the cells keep dividing and dividing. . . and you get unregulated, runaway growth.
Here’s a good visual for the kind of exponential growth we’re talking about (though the video shows quickly-dividing bacteria, and the cells we’re talking about divide much more slowly.)
You can imagine that even something as small as a mammalian cell could start taking up some room if there were enough of them in one area. And this is what a tumor is: a collection of uncontrollably-dividing cells.
If it’s a cancer of blood cells: the cells don’t stay together to form a mass, but they still divide uncontrollably, taking over the bloodstream by sheer numbers and making the fluid equivalent of a “tumor”.
Who gets it?
Anyone.
Old, young. Black, white. Male, female. Educated, uneducated. Anyone who has replicating cells can potentially get cancer. That’s you. That’s everyone you know. That’s everyone you’ll ever meet. Heck, it’s also everyone you’ll never meet!
However, certain types of cancer are more common in certain populations. For example, breast cancer is more common in women then men (although men can also get it). Prostate cancer is exclusively found in men, since women don’t have prostates. Male smokers are 23 times more likely to develop cancer (and not just lung cancer, by the way) than non-smokers. (I don’t have the specific statistic for female smokers, but I’d bet an arm and a leg that it’s similar. And I kinda need both of my arms and legs. Just saying.)
But to be honest, if you need one of your characters to have cancer, you can give them cancer. No matter who they are. I’m not going to call foul.
Why do you get it?
If the DNA of a cell (the blueprints that tell a cell how to act) becomes damaged in such a way that causes the brake mechanisms to fail, the cell may become cancerous. This damage can happen in many ways.
— A person can be born with genes that cause a cell line to become cancerous, such as in familial adenomatous polyposis.
— A person’s environment can cause enough damage that their cells become cancerous, such as with UV exposure and melanoma (a runaway growth of the pigment-containing cells in the skin.) There are also some environmental factors such as the human papillomavirus (HPV) that appear to cause cancer.
— A person can put substances in their body that damage the genes in their cells in a way that causes cancerous growth patterns, such as with smoking and various types of cancer including lung cancer.
— A person can have a genetic predisposition to developing a cancer, but will only develop the cancer if they are also exposed to an environmental factor or toxin.
The way your character gets cancer will probably depend on who your character is, how old, if anyone in their family has had cancer, and what they are exposed to either through their work or their living environment. It’s good to turn to the books to see if any known diseases fit your character type. Again, the National Institute of Health is a good place for this kind of selection research. It has sections on Cancers by Body Location/System, Childhood Cancers, Adolescent and Young Adult Cancers, and Women’s Cancers. It also has a wealth of other information. Go thou and research!
What are typical symptoms of cancer?
You can pretty much figure out what symptoms your character will have based on the function of the organ that has the tumor, and the function of any nearby organ that might be squeezed by a mass of growing cells. Also think about squeezing off a blood supply to a nearby organ, blocking lymphatic drainage, or squeezing the nerves in the area.
If it’s a tumor in the intestines, your character will likely eventually have trouble defecating due to blockage. If it’s a tumor blocking the common bile duct, your character will have symptoms that result from the blockage of the flow of bile and the resultant back-up through the liver: their stool will be gray/white and their urine will be brown, they could have pain on the upper right side of their abdomen (and classically, the pain could radiate to their back), and their skin could turn yellow (jaundice).
Beyond that, there are some classic, non-specific symptoms that many cancers share. Since the uncontrolled cell growth steals a lot of the groceries that the body would rather use to fuel its non-cancerous cells, a person could experience an unexpected and unintended weight loss and fatigue. Cancer cells can release chemicals into the body that generate unexplained fevers as well.
It occurs to me that at this point I should say: Please keep in mind that these symptoms don’t automatically mean you have cancer. They can show up with other diseases, too. If you have a symptom you’re worried about, talk to your doctor about it. It’s his job to sort stuff like that out.
When do you get it?
It’s most common in older populations. According to the American Cancer Society, 77% of all cancers are diagnosed in people age 55 and older.
But that doesn’t mean older people are the only ones who get it. You can give any one of your characters cancer, no matter what their age is.
However, do your research. Some types of cancer are more common in certain age groups. So, pick your organ of choice and look in a pathology text or on the NIH website to see if there’s any particular cancer type known to be likely in your character’s age group.
Where do you get it?
Cancer can happen in any organ. There are some organs that are more likely to develop cancers than others. For example, the heart and eyes are far less likely to develop a neoplasm (although it does still happen).
Here are two graphs showing the most common cancer deaths by year and type of cancer, separated by gender. (Please note that it’s the deaths from cancer that this graph shows, not how common the cancers themselves are. But it might give you a general idea about which organs like to create deadly cancers.)
How fast does it grow? How fast does it spread?
It depends on the type. Some cancers, such as Basal Cell Carcinoma, grow very slowly and are less likely to metastasize (spread to other parts of the body). And some, like melanoma, can grow very fast and spread to every organ system in a person’s body, long before the first symptom presents. It really depends on the type of cancer and where it shows up in the body. Research, research, research. (Sensing a pattern here?)
So, how can you use cancer in fiction?
Pretty much any way you want to, within reason. It’s a good disease type if you need something that develops slowly over years, and isn’t noticed until it’s too late. It’s a good disease type if you need a character to slowly waste away. It’s a good disease type if you need something that could have been cured early, but was missed and so became incurable.
The limits of cancer are pretty much the limits of your imagination. If you want to use a real disease: pick an organ, dig into a pathology text or the NIH and American Cancer Society websites (links in the “Sources” section), and see what’s available.
If you want to invent a cancer. . . well, you can. Pretty easily. Since it’s a mutation away from normal cell function, cancer acts the way cancer feels like acting. As with any other plot point, (1) do your research; (2) your audience will believe the story you tell as long as you justify it; and (3) keep your embellishments quiet and plausible.
Side note: Every once in a while, I see someone’s genius protagonist come up with “a cure for cancer”. It just strikes me as silly. Finding “a cure for cancer” would involve finding a cure for every single individual type of cancer. (Shout-out to medical researchers, by the way, who are devoting their lives to finding cures for every single individual type of cancer!) But please don’t be that writer. Thanks.
Okay, that’s probably enough for now. There’s clearly more to say, but this post is a long one already. Sorry for the choppy read, too.
The contents of this site, such as text, graphics, images, and other material contained on the Site (“Content”) are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this Site!
If you think you may have a medical emergency, call your doctor or 911 immediately. This blog does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the Site. Reliance on any information provided by this blog, or other visitors to the Site is solely at your own risk.
The Site may contain health- or medical-related materials that are sexually explicit. If you find these materials offensive, you may not want to use our Site. The Site and the Content are provided on an “as is” basis.
If you do use this as if it’s medical information, I’ll drop a pebble onto your driveway. The next day, I’ll drop two pebbles. The next day, four. And so on.
Here are all of the fictional poisonings I can name off the top of my head in a minute. (Okay, two minutes. Okay, three.)
The Court Jester (my childhood movie…you Disney kids got nuthin!) Doctor Who (folds in Agatha Christie) Hercules (aka: why you never see Hercules wearing a shirt anymore) Gosford Park (If you haven’t seen it, you must! Excellent ensemble piece.) James Bond (I’m thinking of the one in the poker game; I’m sure there are others too.) Romeo and Juliet (with extra tragedy action!) Rosencrantz and Guildenstern Are Dead (I’m cheating…didn’t want to do two Shakespeare plays in a row, so this is my way around it.) Chuck (spies always like poison) Wizard of Oz (I’m counting the poppies.) Harry Potter (Basilisk!) Lamentation (by Ken Scholes) Batman (Batman!) Socrates (okay, that’s historical, I know. But admit it, it’s fun having Batman and Socrates next to each other on a list.)
Okay, my *mumble* minutes are up. That’s a pretty wide-ranging list, isn’t it?
So poisons are everywhere in the stories we like to tell.
But what exactly is a poison?
It’s a thing you put into someone’s drink that makes them suddenly keel over at the dramatic turning point of your novel!
I’ll let David Tennant tell you how poisons work. (Note: I’m using the long version of this scene not because it’s medically plausible, but because Tennant and Catherine Tate have such a fun comedic dynamic.)
“Something’s inhibiting my enzymes,” says The Doctor.
Enzymes are proteins that are basically little molecular machines that make things happen faster in a molecular reaction. Biochemical processes are just strings of molecular reactions. So, enzymes are proteins that facilitate biochemical processes.
Uh…try that again, please?
Okay. Pretend you have Red Molecule and Blue Molecule, that fit into each other like puzzle pieces to make Purple Molecule. If they were left alone, they’d just bounce off each other in a very molecule-y way, and only rarely manage to bounce into the proper orientation where they click together to become Purple Molecule.
Enter Enzyme McAwesome.
Enzyme McAwesome is a protein that’s wrapped into a configuration that’s designed specifically to grab Red Molecule. When it grabs Red Molecule, the presence of Red Molecule makes the structure of Enzyme McAwesome change so that it now has a part that loves to grab Blue Molecule. When it grabs Blue Molecule, the presence of Blue Molecule changes the structure again so that Enzyme McAwesome slams Red Molecule and Blue Molecule together, in exactly the right orientation to make Purple Molecule. Then Enzyme McAwesome lets go of Purple Molecule, and is ready to grab another Red Molecule and start the process all over again.
If something inhibits Enzyme McAwesome, Red Molecule and Blue Molecule don’t get together quite as fast as they would with the help of Enzyme McAwesome.
Now say that Enzyme McAwesome catalyzes the vital step in a biochemical pathway that creates ATP, the molecule that stores energy for use in molecular actions. If Enzyme McAwesome is inhibited, ATP gets created much, MUCH slower than it would with Enzyme McAwesome’s help. The cell doesn’t make as much ATP as it’s used to making, and so molecular actions are far less likely to be “funded” in an energy-supplying way. If molecular actions don’t get the energy they need to actually action, the cell shuts down. And there’s the end of the cell.
Organs are made up of cells. If enough cells shut down in an organ, the organ will fail. And if enough organs fail in the human body (or the wrong single organ fails), the person will die.
See what poisons are now? Poisons are simply substances that interfere with important biochemical pathways. They basically throw a block in the marble run, causing backups and overflows, and getting in the way of anything getting where it’s supposed to get. Sometimes they will block a branch of a biochemical pathway and direct the substrates down a secondary path where they create toxic molecules which then go on to make trouble of their own.
Poisons can be pretty much anything.
Lead causes problems by binding to enzymatic, receptor, and structural proteins. It is also structurally similar enough to calcium to interfere with metabolic pathways that use calcium. This makes problems in particular in the mitochondria, the “powerhouse” of the cell where most of the ATP is generated.
Cyanide “poisons” the electron transport chain, which is a vital component of the biochemical process that makes ATP using glycolysis and the Kreb Cycle. It basically passes off the extra electrons from the process to an oxygen molecule, which then combines with hydrogen to make water. If the electron transport chain is inhibited, the electrons don’t get passed along, and the marble run starts to back up. And then ATP just doesn’t get made aerobically (that is, with the help of oxygen) (that is, the most efficient way to make ATP); the substrates get shunted to the anaerobic pathway (the one that doesn’t require oxygen). That pathway makes less ATP, and also generates lactic acid, which is what you can feel burning in your muscles when you’re exercising beyond your oxygen supply.
This picture is a graphic representation of the Electron Transport Chain, an important series of membrane proteins in mitochondria that help facilitate ATP production. See the blue words with the 'T' shapes pointing out from them? Those are poisons, and the crossbar of the 'T' points to where they interfere with the Electron Transport Chain. Cyanide is the one labeled 'KCN', which is 'potassium cyanide'.
Warfarin is a fun example because it’s a poison…that’s used as a medicine! It was historically used as rat poison. Now it’s used as a blood thinner. Basically, warfarin interferes with the Vitamin-K-dependent formation of gamma-carboxyglutamate, which is essential for the proper function of a number of clotting factors. The upshot is, warfarin “poisons” the pathway that makes clotting factors, which basically “poisons” the clotting cascade. This can be helpful for people who are at risk for conditions relating to over-clot-ification, such as pulmonary embolism and stroke. This can also be very harmful if it’s not carefully monitored.
There's that 'T' shape again, telling you where warfarin interferes with the process. The negative signs also indicate interference or antagonism, and the positive sign indicates facilitation or agonism.
Water can even act as a poison, if there’s too much of it in your system!
So I’m a little unsure about how to advise you to approach poisons in your fiction. I’m sure you can see that poisons are very, very biochemistry-oriented, so it may be difficult as a layperson to navigate the whole poisoning thing in a completely medically accurate way. So you might want to go the way of the not-precisely-medically-accurate-but-at-least-medically-plausible.
Here are a couple of tips to help you out:
-Pick an organ system (like the gastrointestinal system or the neuromuscular system), and keep the symptoms of the poisoning to that organ system. It helps you organize the symptoms instead of flying all over the map in a medically-implausible way.
-Poisons can hit many organ systems at once, but try to keep symptoms to a minimum; if your character turns blue, their hair falls out, their tongue cramps into a ball, their eyeballs pop out, their heart skips every third beat, and they start pooping blood….well, people are going to start rolling their eyes. But if your character gets poisoned and slowly develops vague stomach problems that get worse and worse and worse until she dies in writhing agony…..that’s a little more plausible.
-This is another situation in which lack-of-specificity is your friend. Non-specific symptoms such as gastrointestinal distress (nausea, vomiting, diarrhea), headache, and/or muscle weakness are good ways of avoiding pitfalls of non-believability. You can add them to specific symptoms, but again, think about keeping your specific symptoms to maybe one or two, and fill any “this-doesn’t-look-serious-enough” gaps with non-specific symptoms.
-If you find yourself at a loss, try modeling the symptoms for your made-up poison after a real-life poison. (You don’t have to name the real-life poison in your work; just steal the symptoms. Although, many medical people will be able to recognize which poison you’re borrowing from. Just keep that in mind.) This will help you organize the symptoms to a biochemical distribution without actually having to understand the biochemistry.
For the more biochemically adventurous:
-Try and figure out which cellular process it’s going to interfere with. Remember that cells need food (glucose), oxygen, and water and electrolytes in physiological balance. Some types of cells need to replicate in order to perform their function; all cells need their replication controlled by regulator proteins or else they become cancerous. Many cells are triggered to certain actions by chemical signaling in the body, and many cells are inhibited from performing certain actions by chemical signals. And on and on and on. You can pick any one of these functions to “poison”.
-Try to decide which organs might be most affected by the process you’ve chosen. If you’re interfering with glucose uptake, the brain will be very strongly affected since it’s dependent on glucose and can’t survive on nutritional substitutes (such as ketone bodies) like most other cells can.
-The liver and the kidneys are usually responsible for cleaning poisons out of the blood, so many poisons will hit the liver and/or kidneys hard.
-Try to match the symptoms of the poisoning to the organ system involved. A person with carbon monoxide poisoning won’t necessarily gasp for air, but they’ll be suffocating on a cellular level. A person with an overdose of warfarin will have trouble with bleeding issues; they’ll bruise easily and get nosebleeds and hemorrhagic strokes and all those other things that go along with not being able to clot your blood.
Okay, I think that’s enough from me for now. Where have you seen fictional poisonings? What makes them seem more or less plausible to you?
The contents of this site, such as text, graphics, images, and other material contained on the Site (“Content”) are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this Site!
If you think you may have a medical emergency, call your doctor or 911 immediately. This blog does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the Site. Reliance on any information provided by this blog, or other visitors to the Site is solely at your own risk.
The Site may contain health- or medical-related materials that are sexually explicit. If you find these materials offensive, you may not want to use our Site. The Site and the Content are provided on an “as is” basis.
If you use this as if it were real medical information, I’ll make YOU fight Sir Griswold. (Good stock!)
So apparently some ignorant douchebag somewhere told the poor people who have to listen to him that immodest women are the cause of earthquakes.
Even though everyone knows that ignorant douchebags are really what cause earthquakes.
Actually, that might not be the case. Earthquakes would be far more common if it were.
But anyway, the blogosphere answers today with Boobquake. Today, women everywhere will be showing a little more cleavage than usual in an order to scientifically expose this theory for the misogynistic bullshit it is.
And, being a uniquely internet-based entity, here’s the only way I could think of to contribute.
Ladies and gentlemen, I give you…THE MAMMARY GLANDS!
Ah, mammary glands! Those fleshy sacks of exocrine tissue that drive men wild! (And some women! And not all men!)
So what are they?
Well. They’re the means by which a woman becomes a food source.
No. Not like that.
Come on. You know what I mean.
Wow. It took three tries.
::sigh::
Anyway.
Here’s the way breasts work.
Anatomy
A breast is composed of a collection of lobes, the functional unit of the mammary gland. Like many other structures in the human body, a lobe looks a lot like a tree:
This is what a lobe of the breast looks like under a microscope.
(Side note: They look a little like alveoli, the air sacs in the lung, don’t they?)
The round structures at the end are exocrine glands (glands that stay connected to the surface that they developed from; for practical purposes, that usually means that they secrete material through a duct). These particular glands secrete milk when a woman is lactating.
The glands of the lobe are connected to each other by a series of ducts, called lactiferous ducts. (lacto = milk, fer = to bear or to carry) You can see the ducts in the picture above; they’re those branch-like structures. As the lactiferous duct gets closer to the nipple, it dilates into a pouch called the lactiferous sinus. You can see it in this picture:
And then all of the lactiferous ducts have an open end at the nipple, where the secretions of the lobes can be expressed to the outside of the body.
And, you know, feed a baby.
These structures are suspended in fat and connective tissue.
Physiology
Breasts are cool and unique, because they aren’t fully formed at birth, and they go through a number of changes in response to reproductive cycles.
Both men and women have a duct system in their breasts. During puberty, a woman’s breasts begin to form lobules at the end of their terminal ducts. Her breasts are very responsive to changes in her internal hormonal environment, particularly the influence of estrogen and progesterone during her menstrual cycle.
These pictures show the Tanner stages of breast development. They can be used to determine a girl's progression through puberty, as well as help diagnose a number of different hormonal disturbances.
A man’s breasts will not develop in the same way, unless he has a hormonal disturbance which causes his breasts to grow. This is called gynecomastia. Some causes of gynecomastia include liver cirrhosis, drug use, steroids, and testicular tumors.
Bob from Fight Club suffered from gynecomastia.
Functional role
If a woman becomes pregnant, her breasts will respond to that hormonal environment as well; they will undergo even more changes to prepare for the eventual feeding of her baby. When the baby is born, the breasts produce a substance called colostrum, which is high in protein and immunoglobulins. After about a week, the colostrum changes to milk, which has a higher fat and calorie content.
In addition to providing the perfect food balance for the baby, breastmilk is also very important to the development of the baby’s immune system. Breastmilk contains IgA, a protective immunoglobulin that is found in the secretions of the body, as well as a number of other components that help support the baby’s own developing immune system.
And all of this happens without anyone having to think about it too much (in the absence of medical problems, of course). All mom and baby have to do is bond with each other, and let the breasts do all the work!
Aren’t breasts awesome?
In conclusion
These fabulous structures are what separate mammals from the rest of the animal kingdoms. They’re cool, they’re important, and they will probably be a little more visible today than usual.
So hooray for breasts! Hooray for empowered women! And hooray for the fact that I live in a society that allows women to show or not show their breasts AS THEY CHOOSE FOR THEMSELVES!
I don’t know about you, but that sure rocks my world!
Happy Boobquake, everyone!
References:
Robbins and Cotran. Pathologic Basis of Disease. 7th edition. Elsevier, 2005
Junqueira, Luis Carlos; Carneiro, Jose. Basic Histology: text and atlas. 11th edition. McGraw-Hill, 2005.
Pictures:
The contents of this site, such as text, graphics, images, and other material contained on the Site (“Content”) are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this Site!
If you think you may have a medical emergency, call your doctor or 911 immediately. This blog does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the Site. Reliance on any information provided by this blog, or other visitors to the Site is solely at your own risk.
The Site may contain health- or medical-related materials that are sexually explicit. If you find these materials offensive, you may not want to use our Site. The Site and the Content are provided on an “as is” basis.
If you use this as if it were real medical information, you will cause an earthquake. So just don’t.
“(The heart), nurtured in the seas of rebounding blood,
where most especially is what is called thought by humans,
for the blood round the heart in humans is thought.” –Empedocles
If you held a gun to my head and asked me what my favorite organ was, I’d probably crap my pants and beg you not to shoot me.
But if you were really serious about getting an answer to your question, I’d probably tell you that I absolutely love the heart. You know, after you took the gun away and I got cleaned up a little bit.
Not just because it pulled a fast one on some of my favorite philosophers. Though I gotta admit, I do love watching the history of knowledge unfold through trial-and-error. But seriously, I think it’s functionally and aesthetically the prettiest organ in the body.
(Kidneys are cool, too, but I get a complex about brainless objects that are nonetheless smarter than I am.)
Wanna see something beautiful?
This shows an MRI of a heart beating. Just watch it for a minute. It’s gorgeous. PS: Can you identify the piano piece? Thanks, Interwebz!
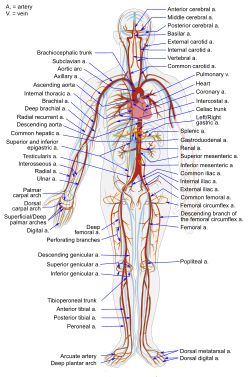
Your heart is basically a chunk of muscle that contracts in a really cool way to push your blood around your body. The heart is the center of the circulatory system. That’s the system that’s responsible for getting important groceries from one place to the other in your body: glucose (cell food), oxygen, etc. It also takes out the trash: urea, carbon dioxide, and all those other yuckies that would otherwise gum up the works. And poison you and stuff. Basically, anything that needs to get from one place to another goes through the circulatory system.
It’s like the internet and the transportation system combined: it’s a series of tubes! And through the tubes goes everything from gasses to sugars to hormonal messages.
What’s the setup for the body’s circulation?
The circulatory system is organized like an infinity sign or a figure-eight, with the heart at the cross-over point. One loop is the pulmonary loop that goes to the lungs, and the other is the systemic loop that goes to the rest of the body and all of the organs.
Okay, now we’re red blood cells! We’re going to take a trip through the circulatory system!
Can we go to Hawaii instead?
No.
Why not?
Because we’re red blood cells. And we’re going to take a trip through the circulatory system.
There are red blood cells in Hawaii. And, if I recall correctly, there are also circulatory systems in Hawaii.
. . .
. . . You’re right.
Yes. Yes, I am.
Okay, then. We’re red blood cells. In Hawaii.
Hooray!
Let’s arbitrarily start our journey right before we get into the heart.
Our job as red blood cells is to carry oxygen (O2). We’ve just popped the O2 off of our hemoglobin at our last stop, and loaded up with carbon dioxide (CO2). We want to get the CO2 out of the body, and pick up some more oxygen so we can make another delivery.
We enter the heart through a big vein called the vena cava. The vena cava empties into the first chamber of the heart, the right atrium.
The right atrium is a little room made of contracting muscle. Its job is to top off the right ventricle, which is the main pumping chamber of the right side of the heart. The atrium and ventricle are separated by a one-way “door” called the tricuspid valve (so called because it has three “cusps”, or leaflets.)
So, the right atrium is going to give a squeeze, and propel us through the tricuspid valve into the right ventricle. The right ventricle is relaxing after its previous squeeze; that’s called “diastole”.
It’s very. . . um. . . muscular in here.
Yeah, these pumping chambers are made completely of bundles of muscle fibers. That’s important, because the heart needs to put some force behind its squeezes.
The right ventricle’s job is to provide the force that pushes us through to the lungs, so we can exchange our load of CO2 for O2. To get there, we have to go through another one-way “door” called the pulmonic valve, and through a series of splitting tubes called the pulmonary arteries.
Note: Some people are taught that “arteries carry oxygenated blood and veins carry de-oxygenated blood.” This isn’t entirely correct. By definition, arteries carry blood away from the heart and veins carry blood toward the heart. In the pulmonary (lung) circulation, arteries carry de-oxygenated blood, and veins carry oxygenated blood.
So the right ventricle gives a good squeeze! This is called “systole”. And now, we shoot through the pulmonic valve. We travel through the pulmonary arteries, and end up in the tree-branch-like system of the capillaries of the lungs.
These capillaries are tiny blood vessels that are only wide enough to let one blood cell through at a time. So let’s hold hands so we don’t lose each other, and squeeze on through. We’re close enough to the alveoli (the tiny bags that fill with air when you breathe) that we can drop off our CO2, and load up some O2 for our next delivery run.
Alveoli
And now we’re set to move on!
After we traverse the capillaries, we find ourselves in a reverse-tree-branch-like system: the tiny capillaries are coalescing to form larger and fewer vessels, called the pulmonary veins. We’re on our way back to the heart!
When we reach the “trunk of the tree”, we’re in the pulmonary vein. This empties into the left atrium. The function of the left atrium is a lot like the function of the right atrium. Its job is to top off the left ventricle.
The one-way “door” between the left atrium and the left ventricle is called the mitral valve. So, the left atrium is going to give a good squeeze, and push us through the mitral valve into the left ventricle. The left ventricle is relaxing; it’s in diastole.
And we’re stunned. We’re just flabbergasted.
Um…why?
Remember the right ventricle? The main pumping chamber that pushed us into the lungs?
Yeah?
It was pretty strong, right?
Yeah, it gave us a good push. It took some force to do that.
Well, strength-wise, the left ventricle could EAT THE RIGHT VENTRICLE FOR BREAKFAST. You know, not even breakfast. Maybe even just a midmorning snack. The left ventricle is HUGE!
Look how much bigger the Left Ventricle is on cross-section!
Maybe it’s compensating for something.
Yeah, it is! It’s compensating for the fact that it has to provide enough force to squeeze blood THROUGH THE ENTIRE BODY!
eep.
So we’ve just come through the mitral valve, and we’re chilling in the left ventricle. In front of us, we can see the aortic valve, which is the one-way “door” that leads out of the heart into the main artery of the body, the aorta.
And I can feel the left ventricle getting ready to squeeze. Get ready for systole!
Um . . .
It’s building up! It’s gonna be a big one!
Ummm. . .
What? What’s wrong?
Stop the circulatory system! I wanna get off!
Too late! Hold on, we’re into SYSTOLEEEEEEEEEEEEE!!!!!!!!!!!!!!!!!!!
AAAAAAAAAAAAAAAAAAA!!!!!!!!!!!!!!!
Observe my sloppy Photoshopping on the way!
We’re sailing through the aortic valve and into the aorta! We have a lot of places we can go to deliver our oxygen now, and our first choice comes up almost immediately: the coronary arteries, which supply oxygen to the heart muscle. These guys are really important; if they get blocked off, you get a myocardial infarction (myo = muscle, card = heart, infarct = oxygen deprivation), also known as a heart attack.
But there’s plenty of blood heading into the coronary arteries; let’s stick with the aorta for a bit.
The Aorta has many branches; each one is an artery going to a different part of the body. The carotid arteries head up to the brain. The renal arteries come off of the aorta as it descends into the abdomen, and supply the kidneys. Just look at all these options!
So, pick a part of the body, and we’ll go there and dump our O2. Then we’ll pick up any CO2 it needs to get rid of.
Let’s go to the fourth toe on the right foot.
Um…sure. Good a place as any, I guess. Any particular reason?
How often does that guy get any attention?
Okay, fair enough. So we’re going to travel through the arterial tree, traveling through smaller and smaller arteries until we reach the bed of capillaries that supplies the (ahem) fourth toe on the right foot. Each cell is within striking distance of a capillary, so it can have access to supplies and waste removal services.
Now pick a cell and unload your O2 so it can keep doing its job. And go ahead and pick up some CO2, too.
Got it. Let’s blow this popsicle stand.
Awesome!
So, now we’re going to head out the other side of the capillary bed. The blood vessels are coalescing again, making bigger and bigger vessels. This is the venous part of the systemic circuit.
venous?
Venous.
Venous!
Hee hee! VENOUS!
VENOUS!
Okay, okay, you win. I can’t shout any louder without getting people confused as to who’s talking.
Ooh, self-referential font humor. I’ll declare victory anyway.
Good job.
Okay, we’re headed through the veins on the way back to the heart. The veins coalesce into the vena cava. . . and we’re back where we started.
From here, we’d pass through the right heart into the pulmonary circuit, and then pass through the left heart into the systemic circuit, and around and around and around.
But that would make me a little dizzy, and plus, this post is a monster as it is.
So, that’s the mechanical setup of the circulatory system. It’s just a series of pumps and pipes. If you want to mess with it. . . just think about what happens when a system of pipes gets backed up. Or if the valves start allowing back-flow, or if they get too stiff to allow much flow. Or if the pump becomes weak and inefficient. Or if the pressure gets too high for the pump to push against.
But before I sign off for today, wanna see something gorgeous?
This is the procedure I spent the vast majority of last month observing. It’s called a cardiac catheterization. We’re taking pictures of the coronary arteries by shooting a little bit of opaque dye into them under an X-ray machine. This test looks for blocked or narrowed coronary arteries, which could cause a heart attack if they’re not opened up.
Man, I could look at those forever.
What’s your favorite organ system?
Source:
Cohen, Curd, and Reeve. Readings in Ancient Greek Philosophy. Second edition. Hackett Publishing Company, 2000.
Pictures:
The contents of this site, such as text, graphics, images, and other material contained on the Site (“Content”) are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this Site!
If you think you may have a medical emergency, call your doctor or 911 immediately. This blog does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the Site. Reliance on any information provided by this blog, or other visitors to the Site is solely at your own risk.
The Site may contain health- or medical-related materials that are sexually explicit. If you find these materials offensive, you may not want to use our Site. The Site and the Content are provided on an “as is” basis.
If you use this as if it were real medical information, I’ll take my circulatory system to Hawaii without you.
“Tools for the Toolbox” is a series of posts that describe disease types and organ systems. Eventually I hope to include enough information that a writer might be able to do some creative mixing and matching to produce the symptoms they want to give a character. Because it’s really frustrating to throw darts in the dark and hope something lands near the bull’s-eye. Hope it helps!
I’ll start this discussion of viruses by saying that Virology is a field of study in and of itself. So there’s no way that this blog post is going to come even close to being comprehensive or even extensive. I’m doing highlights only, and I may post further information at a later date.
Viruses act in a huge variety of different ways. So instead of talking about individual viruses and what they do, let’s talk about HOW they do what they do.
Viruses don’t have much of a life. As a matter of fact, they aren’t really alive. They’re just tiny organic machines that exist to make copies of themselves. If that doesn’t get your sci-fi juices flowing by itself, check your pulse. Or your level of consciousness.
Let’s build a virus!
So. In order to make copies of a thing, you need an original. In the case of viruses, the “original” copy is a strand of genetic material. It will be DNA or RNA, but not both. Regardless, the genetic material contains instructions for making a new virus, just like human DNA contains the instructions for making a human being. This picture shows DNA and RNA, side-by-side for comparison.
So, now we have a strand of genetic material. Let’s roll it up into a ball, and stuff it into a pouch made of proteins. This pouch or coat is called a “capsid”.
The genetic material (DNA or RNA) would be contained inside. Some capsids carry structural proteins and enzymes within the coat. Pretty handy, since there’s not much room inside. (Viruses are small! Like, really small!)
And for some viruses, that’s all they bother with. They’re called naked viruses.
OoooooooOOOOooooooooh!
Settle down. (Rhinoviruses are such teases.)
Other viruses are a little more modest. In addition to their capsid/coat of proteins, they also like to give themselves an extra layer. This is known as an “envelope”, and is made of a “lipid bilayer”, which is what the cell membranes of our cells are made of. It looks like this:
You can see the genetic material, coated by the capsid, enveloped by the envelope.
So, now we have a virus.
The driving purpose of a virus… THE VERY REASON FOR ITS EXISTENCE… is to make copies of itself. But it can’t! It’s a strand of genetic fluff wrapped in one or two layers. It doesn’t carry the proper materials or machinery to make copies. Doesn’t that suck?
Um…I’m not really worried about the existential satisfaction of the common cold.
Me either, to be honest. But it does really suck. Because instead of throwing up its non-existent hands at its complete and utter lack of purpose-fulfilling-equipment, it decides to hijack someone else’s.
Namely, yours.
I have viral-purpose-fulfilling-equipment?
Yup. The cells in your body contain the equipment for replicating genetic material. And the virus wants it!
So, here’s the virus’s rather overdramatic modus operandi. It drifts around, aimless and without propulsion, until it lands by chance on a cell. Then, it injects its genetic material into the cell! It’s like hijacking a factory and replacing its blueprints with your own. (Not, I feel I should point out, that I’ve ever hijacked a factory or replaced its blueprints with my own.)
Particularly not this factory. Or its blueprints.
Anyway, the cell then turns into a virus-producing factory! It’s forced to use its own machinery and resources to make hundreds and hundreds of viruses! As a matter of fact, the cell-factory is pushed into overdrive by its hijackers, and eventually so many viruses are created that there’s just no room in the cell anymore. So the cell EXPLODES, spraying new, copied viruses everywhere!
And then it all begins again.
A little diabolical, no?
Aren’t there any defenses built into the cell? Viruses have been around for a long time, after all.
Well, kinda. Once infected, the cell is pretty much a goner. But that doesn’t mean it gives up. During the hijacking/infection process, the hijacked cell displays some of the viral proteins on the outside of its membrane. It’s like sending up a panic flag. This alerts the rest of the body that the cell has been infected. The flag also gives information about the infecting agent to other cells nearby so they can get their defenses up, and sends a message to the immune system that there’s an attack going on.
It’s a really nifty process, and its ingeniousness blows me away. (I love the immune system, though learning it the first time really sucked monkey balls! I blame the naming scheme. Everything and its brother was named CD28 or CD32 or whatever. Almost impossible to keep straight.)
Who gets viruses?
Everyone.
Different people get exposed to different viruses, though. As with any other illness (besides genetic and autoimmune diseases), the types of viruses you’re exposed to depends on your surroundings and your lifestyle. A few examples:
– Human Papillomavirus (HPV) is spread through sexual contact.
– Cruise ships, dormitories, and nursing homes are great places to catch the Norwalk virus.
– Poliovirus is more likely found in areas of poor sanitation.
– Drug abusers who inject substances into their bloodstream are at risk for Human Immunodeficiency Virus (HIV) and Hepatitis B and C.
Different people also have different ways of responding to viruses. Some people might catch it and pass it along without developing any symptoms at all, while other people may be laid up for days or even die from the infection.
For example, Respiratory Syncytial Virus (RSV) causes a slight head-cold in adults…but can cause a life-threatening bronchiolitis (infection of the bronchioles in the lungs) in infants.
What are typical symptoms?
Depends on the virus.
You got your “flu-like symptoms” for your respiratory viruses: Fever, cough, sore throat, runny nose, headache, body aches, chills, fatigue, etc.
You got your fun vomiting-and-diarrhea pattern for your gastrointestinal viruses.
You got your lymphadenopathy-plus-sore-throat-and-fever pattern for Epstein-Barr virus (mononucleosis, or just “mono”) and the initial stage of HIV infection. (lymphadenopathy = swollen lymph nodes)
There are others as well.
And then the virus can kinda do its own thing from there. HIV attacks the T cells of the immune system. Mumps also likes the T cells for an initial replication site, then heads over to other tissues like the salivary glands and the testes. Herpes viruses (which include everything from cold sores to chicken pox/shingles to painful genital rashes) like to camp out in nerve ganglia when they’re done with their initial infection. Then they flare up in the distribution of the nerves they’re hiding in whenever the fluctuations of the body’s immune system give it a chance. (ganglia = collections of nerve cell bodies)
Basically, you can model your virus on any of the above patterns, and then let it attack your character in any way you want it to. But remember that it’s more plausible to start with a few, easily explained symptoms within the same body system (neurological, gastrointestinal, respiratory, etc.) than it is to justify a total, multi-system shutdown immediately on infection. The multi-system shutdown can happen, certainly…but let it build up.
Note: Sometimes a virus’s symptoms will correlate with the method of spread. For example, the rhinovirus (common cold) is spread through the air and causes respiratory symptoms. Norwalk virus is spread through the fecal-oral route (that’s exactly what it sounds like…) and causes gastrointestinal symptoms. HIV is spread through blood and fluid contact, and it attacks white blood cells. Many viruses don’t follow these kinds of patterns, but it’s something to think about when you’re world-building.
How do you cure them?
Well, that’s a tough one. There are antiviral medications that interfere with the life cycle of a virus and minimize the damage an infection can cause, but viruses themselves aren’t really cooperative when it comes to general medical treatment.
Usually, medical personnel defer to “supportive treatment” when dealing with viruses. That is, keeping the symptoms of infection under control while the body’s immune system mounts its own defense and fights off the infection itself. If a baby has severe diarrhea and vomiting during his bout of viral gastroenteritis, he should be hospitalized so his fluids can be replaced. If a college student develops respiratory distress from an influenza infection, his breathing can be supported with a ventilator. And so on.
Antibiotics have absolutely no effect on viruses.
But Good Housekeeping told me that…
Antibiotics have absolutely no effect on viruses.
But I took penicillin once for…
ANTIBIOTICS HAVE ABSOLUTELY NO EFFECT ON VIRUSES.
Do we have any questions about antibiotics and whether or not they have any effect on viruses?
. . .
Good. Please don’t come into my office and demand I give you antibiotics for your viral infection. Please don’t come into my office and demand I give your child antibiotics for her viral infection. This happens way too often, and it really pisses me off. It’s actually one of the reasons I decided not to go into Pediatrics as a specialty, and why I hope to avoid outpatient medicine as much as possible.
Some ways to use viruses in fiction.
-Use a virus if you need an epidemic that spreads quickly, like Captain Trips in The Stand.
-Use a gentled virus as a tool for altering genetic material, like they do with gene therapy.
-Use a virus if you want to create superbacteria in a population, since a population that incorrectly takes antibiotics for viral infections will teach its bacteria how to resist any medicine it’s exposed to. Like with MRSA. Or A. Baumannii, which killed my grandfather. (Yes, this is NOT some science fictional concept, and this is NOT some fuzzy problem that we’re just passing off to our children to solve later. This is killing people RIGHT NOW. Really, really IMPORTANT people. Is your grandfather next?)
-Use a virus if you need a disease that quickly mutates. This could prevent even your genius protagonist from coming up with a cure, or could make any treatments that she cooks up completely ineffective, just in time for your exciting climax. Like with HIV or influenza.
So, viruses are pretty diabolical little buggers. Versatile diabolical little buggers. And let’s be honest: what story doesn’t need a good bit of diabolical in it? Or a good bit of versatility?
The contents of this site, such as text, graphics, images, and other material contained on the Site (“Content”) are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this Site!
If you think you may have a medical emergency, call your doctor or 911 immediately. This blog does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the Site. Reliance on any information provided by this blog, or other visitors to the Site is solely at your own risk.
The Site may contain health- or medical-related materials that are sexually explicit. If you find these materials offensive, you may not want to use our Site. The Site and the Content are provided on an “as is” basis.
If you use this as if it were real medical information, I will hijack your factory, and replace its blueprints with my own. Because I’m diabolical like that. And rather versatile.






















































.svg/350px-Diagram_of_the_human_heart_(cropped).svg.png)