(Well, I could do without the obnoxious laugh track. Things like this were so much funnier to me before I started with the whole medical training thing. Now all I can think about is how much their medical bills are going to be.)
(Anyway. Article.)
We see fainting everywhere in fiction, from swooning damsels in distress to buffoons scraping for cheap laughs in mindless comedies. And heroes are always fighting off a loss of consciousness when they’re being tortured by evil bad dudes everywhere, and annoying sidekicks are always dropping into the nearest pile of horse puckey at the sight of blood.
So what’s going on? Is there a medical explanation?
Of course! 😀
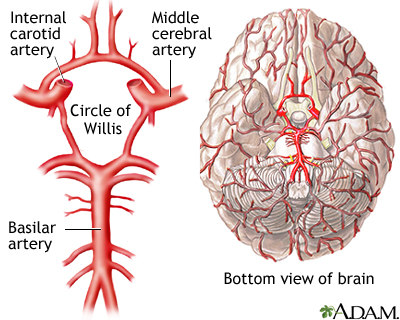
If your brain doesn’t get enough blood flow, it’ll shut down. And this causes a person to lose consciousness. That’s called syncope. If they’re upright, they’ll fall down. (If they don’t lose consciousness, but still experience dizziness and other near-syncope-like symptoms, it’s called….near-syncope. Thought it was going to be more dramatic, didn’t you? 😀 ) True syncope is also characterized by a relatively quick recovery, with no real neurological after-effects.
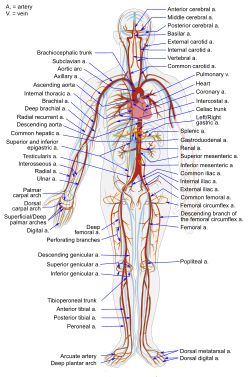
So, listen. Gravity is always pulling your blood down toward the center of the earth. Your cardiovascular system is all set up to fight against this force to keep the blood circulating adequately to all parts of your body, no matter what orientation it’s in. It’s a rockin’ system.
But if something goes wrong with the cardiovascular compensation against gravity, gravity wins. And the blood gets pulled away from whatever is the highest part of the body. If it’s your brain, your brain will shut down until enough blood gets back into it.
As a side note: fainting sure isn’t fun, but it’s a pretty smart failsafe in case gravity starts winning. It gets you horizontal, on the ground, so your brain is a low enough point that gravity won’t pull too much blood away from it. Cool, huh?
So what causes the failure in the first place?
There are a lot of reasons why people faint. As a matter of fact, I dreaded getting a syncope case during my time-limited practical exam for my boards, because there was SO MUCH WORKUP to do that I’d never get to everything in time. The ultimate cause could be in the heart, or the brain, or the lungs, or an imbalance in the blood…..and it could be any number of causes within those categories. Like I said, lots of reasons.
But how about fainting in fiction? The guy who passes out instead of revealing the secret location of his hidden army while under duress? The girl who can’t stand the sight of needles? The dude that gets overrun by carnivorous spiders because his maladaptive phobia causes him to faint when he should be running away, and thus provides an opportunity for us to see exactly what said carnivorous spiders would do to our erstwhile hero if they could manage to outsmart her? The poor folks in the wedding videos?
It’s probably all from the same end cause: vasovagal syncope.
Say what now?
Vasovagal (vaso – blood vessels, vagal – having to do with the vagal nerve and parasympathetic function) syncope (fainting).
This can happen with a strong emotional shock, or with a large, sudden amount of pain.
Here’s what happens. The sympathetic and parasympathetic influences are in their tug-of-war balance, keeping heart rate, blood pressure, breathing rate, etc. all around their preferred normal baseline ranges. Suddenly, there’s pain or terror, or something that strongly stimulates the sympathetic branch of the nervous system (the fight-or-flight branch)! The sympathetic tone leaps WAY out of balance, and the tug-of-war leans STRONGLY to the fight-or-flight side.
In reaction to the increased sympathetic tone, the heart contracts HARD! (Remember, in a fight-or-flight situation, it’s a good idea to have more blood pumping through your system.)
Then, sensors in the heart that are supposed to be keeping an eye on the balance between the sympathetic and parasympathetic tone see that the sympathetic tone has completely overwhelmed the parasympathetic tone! And they freak out! They have to balance the discrepancy somehow! So they send signals to increase the parasympathetic (“vagal”) tone!
But then, the overwhelming sympathetic tone reduces to a certain extent, because it was probably a bit of an over-reaction.
Now, all you’re left with is an overwhelming parasympathetic influence, which drags things STRONGLY over to the rest-and-digest side! This means heart rate, blood pressure, etc. all drop like stones. And if your blood pressure drops enough that it can’t pump enough blood to your brain, BAM! Your brain shuts down and you’re on the floor.
Illustrate that point with a random side story!
How funny that you’d encourage me to do such a thing. It’s almost as if we were both internet-based entities being written by a single author for the purpose of increasing the accessibility of a blog post!
I’ve actually experienced vasovagal syncope. Pretty recently, as a matter of fact. In my hapkido class, I was teaching a lower belt how to do a particular combination of a joint lock and throw. And she did it really well. So well, in fact, that she threw me right off the mat. I hit my knee really hard on the floor, and it hurt like crazy.
And then, not realizing that I had just experienced a potentially triggering stimulus, I got up off the floor to show her how to position herself so she didn’t throw me off the mat the next time.
And I started feeling nauseous. And dizzy. And woozy. And a little hot. And what do you know? I actually recognized the symptoms! I felt my pulse, and sure enough, it was much slower than it should have been under the circumstances. And I remember thinking, “If I don’t lie down on the floor RIGHT NOW, I’m going to fall down on the floor.” So I lay down. Just in time.
Every time I tried to sit up, I felt the same faintness. So I stayed down until my body figured out that I was actually okay, and my autonomic nervous system sorted itself back out into its proper balance.
Okay, but this whole explanation doesn’t exactly follow for the wedding videos. I mean, the brides weren’t THAT hideous. Neither were the grooms, for that matter.
Well, there’s something else that causes a vasovagal response.
Nothing.
Literally.
If there’s nothing going on that activates your sympathetic system, your autonomic nervous system gets so bored that the sympathetics just shut down. Your heart rate falls. Your blood pressure falls. You lose tone in your blood vessels, and they dilate to their full extent. Blood falls down through your legs and away from your brain. And bam! You’re on the floor!
This happens to medical students all the time. (A medical student’s job during a surgery is usually to stand and watch. And hold the retractors that pull tissue away from where the surgeon is working. For. Hours. On. End.) One of the first things they told me during my surgery rotation was what to do if I started feeling faint. Because situations like that are very, VERY risky for the whole vasovagal syncope thing.
It also happened to my little brother a lot when we were singing in choir performances under hot lights, doing weird musical-but-non-physiological things with our breathing. It happens to people who are standing in crowds listening to politicians talk. It happens to people standing during a wedding ceremony.
But this all hinges on gravity, right? What about astronauts?
Okay, I gotta drop this in here. I actually don’t know too much about what happens in an actual zero G environment. I can guess. But, I think it’s even more interesting what happens after they get back to Earth.
After a while in zero G, astronauts’ bodies tend to forget their antigravity compensation mechanisms, because the body hasn’t used them for a while. So when they get back into a gravitational environment, they experience orthostatic hypotension for a while until the compensatory mechanisms remember how to kick back in.
Oh, how I loves me some physiology! (Does it show?)
(Anyone else wanna clock that guy at the end, or is it just me?)
Sources:
Ganong, William F. Review of Medical Physiology. 21st edition. McGraw-Hill, 2003.
McDermott, Daniel, et al. Approach to the adult patient with syncope in the emergency department. UpToDate, May 2010. http://www.uptodate.com/online/content/topic.do?topicKey=adult/6980&selectedTitle=1~150&source=search_result
Sabatine, Marc S. Pocket Medicine, 3rd edition. Lippincott Williams & Wilkins, 2008
The contents of this site, such as text, graphics, images, and other material contained on the Site (“Content”) are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this Site!
If you think you may have a medical emergency, call your doctor or 911 immediately. This blog does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the Site. Reliance on any information provided by this blog, or other visitors to the Site is solely at your own risk.
The Site may contain health- or medical-related materials that are sexually explicit. If you find these materials offensive, you may not want to use our Site. The Site and the Content are provided on an “as is” basis.
If you use this as if it were real medical information, I’ll sic gravity on you. Yeah, that’s right. Gravity! What now, mutha-luvah?





























.svg/350px-Diagram_of_the_human_heart_(cropped).svg.png)





{kind=link}